What Actually Happens When You Roll Your Ankle
Most athletes who have rolled an ankle describe the same experience: one moment everything was fine, and the next it wasn’t. There was no time to react, no warning, no chance to brace for impact. The injury simply happened.
That description is more accurate than it might sound. Ankle sprains aren’t slow events that can be avoided by training for faster reflexes. They are among the fastest traumatic injuries in sport—and understanding why is the first step toward understanding what can actually protect against them.
The Anatomy of a Lateral Ankle Sprain
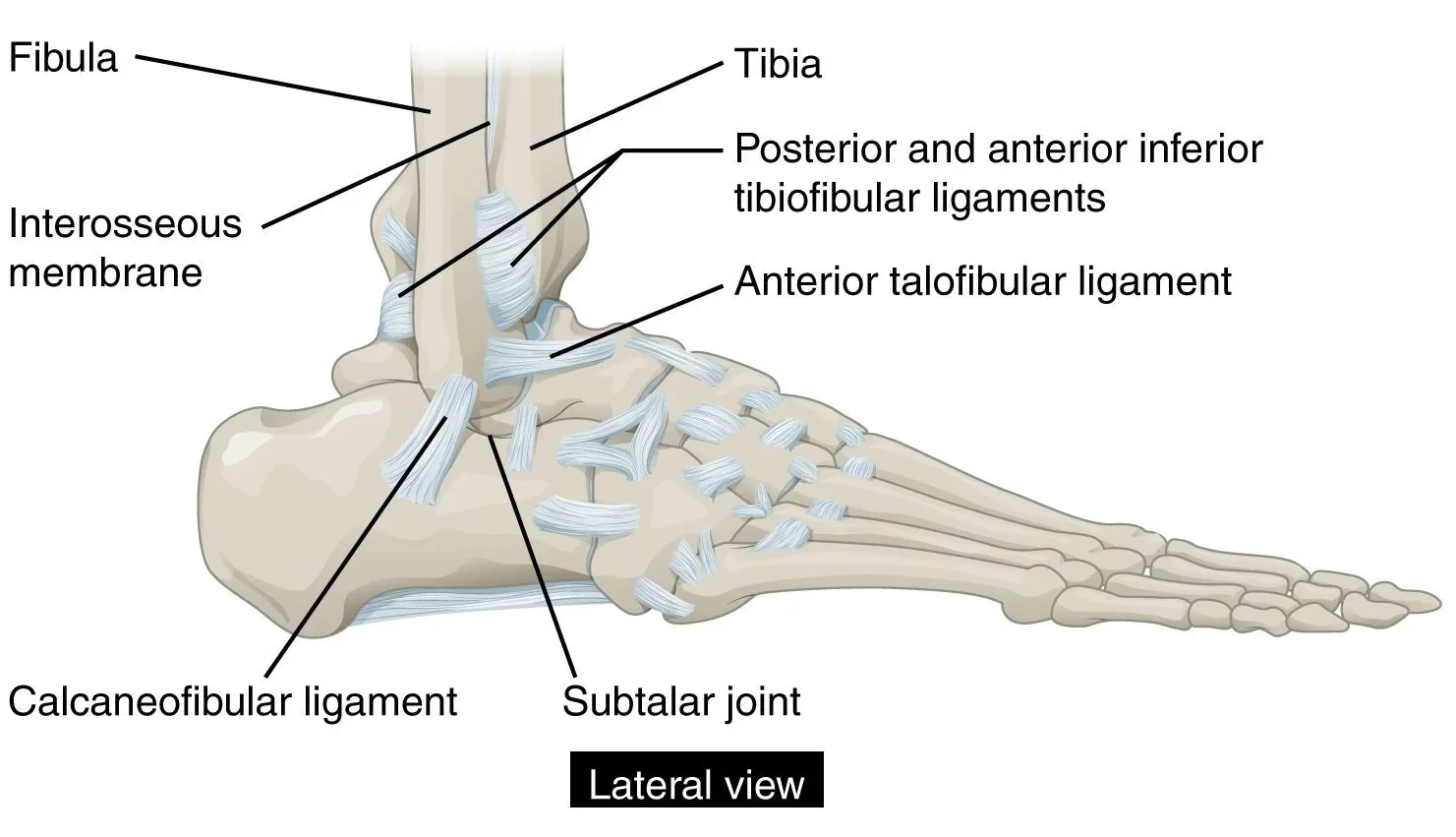
OpenStax College, CC BY 3.0 https://creativecommons.org/licenses/by/3.0, via Wikimedia Commons
The ankle joint is stabilized on its outer side by three ligaments collectively known as the lateral ligament complex. These structures—the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL)—work together to resist the inward rolling motion of the foot known as inversion.¹
These ligaments are not equal partners. The ATFL, which runs from the front of the outer ankle bone (the lateral malleolus) to the talus (the bone where the shin meets the foot), is the thinnest and weakest of the three.²˒³ It is also the most exposed: it bears the primary load when the ankle is pointed downward—exactly the position the foot is in when it plants and rolls during a cut, landing, or change of direction.¹ As a result, the ATFL is involved in roughly 70 percent of ankle sprains.¹
The CFL is stronger than the ATFL and engages more in a neutral or upward-flexed ankle position.¹˒² It comes under load when an inversion force continues after the ATFL has already been compromised. The PTFL is the strongest of the three and is rarely injured in isolation. It typically tears only in the most severe injuries, where the ATFL and CFL have already failed entirely.¹˒³
This sequential failure pattern is important. Most ankle sprains are ATFL injuries. More severe sprains involve the CFL as well. The most severe—true Grade III injuries involving full lateral instability—are those where all three structures have been damaged. Understanding the cascade helps explain why protecting the weakest link matters so much. Stop the ATFL from failing and you stop injury progression in its tracks.
Small Margins
Here is what makes the ATFL’s vulnerability particularly striking. The ligament is typically 20 to 25 millimeters long at rest.⁴ Tissue damage at velocity can begin at a strain of around 3 to 5 percent, which translates to as little as 0.6 to 1.25 millimeters of excess elongation beyond the ligament’s elastic limit.¹˒⁵˒⁶ That’s about the thickness of a paperclip.
That margin is not forgiving. And it gets even smaller under dynamic conditions. Research on ankle ligament mechanics indicates that at the high strain rates seen during sports injuries, tissue becomes stiffer and more brittle, meaning it can fail at the lower end of reported load ranges.⁶˒⁷
The force required to initiate Grade I damage to the ATFL—somewhere in the range of 100 to 140 newtons—is not extreme by athletic standards.¹˒² The ankle routinely experiences ground reaction forces of two to seven times body weight during running and cutting.⁷ The ATFL is not failing because the athlete did something unusual. It is failing because the load arrived faster than the joint’s passive structures could manage.
The Speed Problem
High-speed video analysis of ankle sprain events captured during sporting competition provides some of the clearest data on how fast these injuries actually happen. During normal sporting motion, the ankle inverts at roughly 22 to 85 degrees per second. During documented injury events, that number climbs dramatically. Measured cases in tennis and basketball have recorded inversion velocities of 500 degrees per second and higher, with some events exceeding several times that figure.⁸˒⁹ At those speeds, the ankle can move through a significant range of motion in the literal blink of an eye.
The peroneal muscles, which run along the outer leg and are the body’s primary active defense against ankle inversion, typically show electromyographic activation within 60 to 100 milliseconds after a perturbation is detected, with total motor response taking longer still when electromechanical delay is accounted for.¹⁰ In many inversion injuries, that response arrives after the initial tissue damage has already begun. This is not a failure of athletic preparation or strength. It is simply a fundamental constraint of human neuromuscular latency.
Braces and athletic tape provide passive resistance, but they carry their own limitations: mechanical slack and material compliance mean they begin engaging after the joint has already moved, not at the moment loading begins.⁷ For a ligament where the entire injury threshold may be reached within a millimeter or two of excess elongation, the window that passive devices miss can be the window that matters most.
Sprain Grades: Theory and Practice
Ankle sprains are typically classified into three grades based on the extent of ligament damage.¹˒³
Grade I involves micro-tears and localized tenderness without significant instability. Athletes often describe being able to walk, albeit with discomfort. Return to play with appropriate management is typically measured in days to a couple of weeks.
Grade II involves partial tearing, usually of the ATFL and sometimes the CFL. Swelling and bruising are more significant, and some mechanical instability may be present. Recovery timelines vary but often run several weeks, with meaningful risk of reinjury if the athlete returns to play before adequate healing and neuromuscular rehabilitation is completed.
Grade III represents a complete rupture of one or more ligaments, with frank instability. These injuries require careful management (sometimes surgical) and can sideline athletes for months. They also dramatically increase the risk of chronic ankle instability, a condition in which the lateral structures never fully regain their pre-injury mechanical integrity, leaving the joint vulnerable to repeated sprains.³˒¹¹
The last point bears repeating. Research consistently shows that among athletes with a history of ankle sprains, the prevalence of chronic ankle instability ranges from roughly 40 to 76 percent depending population and sport.¹¹ The first sprain may not be the last.
What Trainers and Athletes Can Take From This
A few practical implications worth carrying onto the training ground:
The speed of an ankle inversion injury means that reaction-time-based prevention—training athletes to avoid rolling their ankles through skills and drills work—has limited effectiveness. Proprioceptive training, balance work, and neuromuscular conditioning are genuinely valuable for reducing injury risk and improving recovery, but their value is more in reducing the frequency of situations where the ankle is put at risk, and in improving the quality of rehabilitation afterward.
Taping and bracing are useful tools, but their limitations are structural, not just practical. They add resistance before the joint moves outside a safe range, but they engage passively and imperfectly.⁷ Athletes who have previously sprained an ankle benefit meaningfully from external support during return to sport, but support is not the same as protection.
Grade I sprains are frequently undertreated. The injury is often written off as minor, and athletes are returned to play too soon, before tissue healing has been adequately addressed. This undertriage is one of the most common contributors to the reinjury cycle that turns a manageably mild first sprain into a persistent problem. Once persistence is established, it is difficult to fully reverse. Therefore, the best intervention for chronic ankle instability is not developing it in the first place.
LigaSys is developing Smart Ligament™ systems — reactive wearable hardware designed to sense dangerous joint motion and respond mechanically in real time. If you're working on athlete availability and performance outcomes, we'd like to hear from you.References
Bergman R, Li D, Shuman VL. Acute Ankle Sprain. [Updated 2025 Aug 2]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. https://www.ncbi.nlm.nih.gov/books/NBK459212/
Attarian DE, McCrackin HJ, DeVito DP, McElhaney JH, Garrett WE Jr. Biomechanical characteristics of human ankle ligaments. Foot & Ankle. 1985;6(2):54–58. https://pubmed.ncbi.nlm.nih.gov/4065775/
Siegler S, Block J, Schneck CD. The mechanical characteristics of the collateral ligaments of the human ankle joint. Foot & Ankle. 1988;8(5):234–242. https://pubmed.ncbi.nlm.nih.gov/3366428/
Khawaji B, Soames R. The anterior talofibular ligament: A detailed morphological study. The Foot. 2015;25(3):141-147. https://www.sciencedirect.com/science/article/pii/S0958259215000371
Nigg BM, Skarvan G, Frank CB, Yeadon MR. Elongation and forces of ankle ligaments in a physiological range of motion. Foot & Ankle. 1990;11(1):30–40. https://pubmed.ncbi.nlm.nih.gov/2210531/
Funk JR, Hall GW, Crandall JR, Pilkey WD. Linear and quasi-linear viscoelastic characterization of ankle ligaments. Journal of Biomechanical Engineering. 2000;122(1):15–22. https://pubmed.ncbi.nlm.nih.gov/10790825/
Rochelle DC, Herber A, Ktistakis I, et al. Mechanical characterisation of the lateral collateral ligament complex of the ankle at realistic sprain-like strain rates. Journal of the Mechanical Behavior of Biomedical Materials. 2020;102:103473. https://www.sciencedirect.com/science/article/abs/pii/S175161611930774X
Fong DTP, Ha SCW, Mok KM, Chan CWL, Chan KM. Kinematics analysis of ankle inversion ligamentous sprain injuries in sports: five cases from televised tennis competitions. American Journal of Sports Medicine. 2012;40(11):2627–2632. https://pubmed.ncbi.nlm.nih.gov/22967824/
Kristianslund E, Bahr R, Krosshaug T. Kinematics and kinetics of an accidental lateral ankle sprain. Journal of Biomechanics. 2011;44(14):2576–2578. https://pubmed.ncbi.nlm.nih.gov/21824618/
Konradsen L, Ravn JB. Ankle instability caused by prolonged peroneal reaction time. Acta Orthopaedica Scandinavica. 1990;61(5):388–390. https://pubmed.ncbi.nlm.nih.gov/2239158/
Hufschmidt A, Mauritz KH. Chronic transformation of muscle in spasticity: a peripheral contribution to increased tone. Journal of Neurology, Neurosurgery & Psychiatry. 1985. https://pubmed.ncbi.nlm.nih.gov/4031912/(See also: Ebig M, et al. The effect of sudden inversion stress on EMG activity of the peroneal and tibialis anterior muscles. Journal of Orthopaedic & Sports Physical Therapy. 1997;25(5):331–337. https://pubmed.ncbi.nlm.nih.gov/9243405/)
Lin CI, Houtenbos S, Lu YH, Mayer F, Wippert PM. The epidemiology of chronic ankle instability with perceived ankle instability: a systematic review. Journal of Foot and Ankle Research. 2021;14:41. https://pmc.ncbi.nlm.nih.gov/articles/PMC8161930/